Timings
-
Mon - Sat
08:00am - 08:00pm


Meniscus of the knee are crescent-shaped wedges that fill the gap between the tibia and femur. The menisci provide joint stability by creating a cup for the femur to sit in. The outer edges are fairly thick while the inner surfaces are thin.
The one on the inner side is called medial meniscus and one on the outer as lateral meniscus. The medial meniscus, located on the inside of the knee, is more of an elongated “C”- shape, as the tibial surface is larger on that side. The medial meniscus is more commonly injured because it is firmly attached to the medial collateral ligament and joint capsule. The lateral meniscus, on the outside of the knee, is more circular in shape. The lateral meniscus is more mobile than the medial meniscus as there is no attachment to the lateral collateral ligament or joint capsule.
The outer edges of each meniscus is attached to the tibia by the short coronary ligaments. Other short ligaments attach the ends of the menisci to the tibial surface. The inner edges are free to move because they are not attached to the bone. This lets the menisci change shape as the joint moves. The front portion of the meniscus is referred to as the anterior horn, the back portion is the posterior horn, and the middle section is the body.
Type of injury depends on location
Location – A tear may be located in the anterior horn, body, or posterior horn. A posterior horn tear is the most common. The meniscus is broken down into the outer, middle, and inner thirds. The area in which the tear is located will determine the ability of the tear to heal, since blood supply in that area is critical to the healing process. Tears in the outer 1/3 have the best chance of healing.
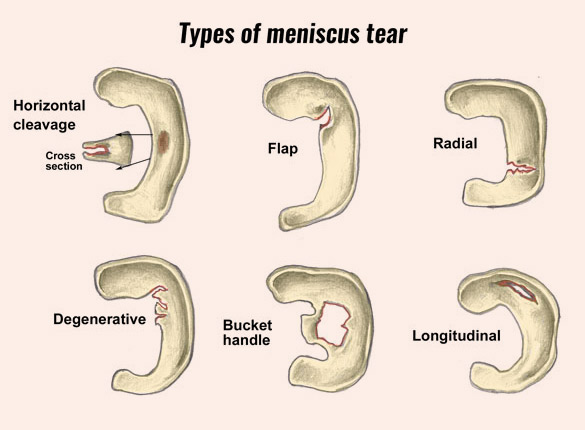
Pattern – Meniscal tears come in many shapes. Examples of the various patterns are:
A complex tear – includes more than one pattern.
Complete tear – A tear is classified as being complete or incomplete. A tear is considered complete if it goes all the way through the meniscus and a piece of the tissue is separated from the rest of the meniscus. If the tear is still partly attached to the body of the meniscus, it is considered incomplete.
Acute tears are often sports related and usually the result of a twisting injury in the younger, active adult population. Symptoms of an acute tear are usually pain, swelling, and movement irregularities. When the tear gets in the way of normal knee motion, the knee can “catch” or “lock” as it moves.
Degenerative tears are more common in the older population. The patient may experience repeated swelling, but often can’t recall any specific injury. The swelling also may be the result of an injury caused by a very minor movement. Mechanical symptoms, such as knee catching or locking, often exist. Or, the patient may simply experience pain.
Non-operative Treatment Many small meniscal tears will heal without surgical treatment. Also, some tears may have no symptoms.
Partial tears, degenerative tears, and stable tears may be observed for 2 – 3 months.
If symptoms disappear, no surgery is needed. The use of a knee brace and restriction of activities may be recommended to prevent further injury.
Surgical Treatment
Surgical treatment for a meniscal tear may be indicated if:
If surgery is recommended, the procedure chosen is usually dependent on the location and type of meniscal tear. Procedure is performed using an arthroscope and usually don’t require an overnight hospital stay.
This procedure is used for stable tears located on the periphery, the meniscus and joint capsule junction, where there’s a good blood supply. Multiple holes or shavings are made in the torn part of the meniscus to promote bleeding, which enhances the healing process.
This surgical procedure is used for tears located in the inner 2/3 of the meniscus where there is no blood supply. The goal is to stabilize the rim of the meniscus by removing as little of the inner meniscus as possible. Only the torn part of the meniscus is removed. If the meniscus remains mostly intact with only the inner portion removed, the patient usually does well and does not develop early arthritis.
This procedure involves the complete removal of the damaged meniscus. This technique is not performed now a days. Removal of the entire meniscus frequently leads to the development of arthritis.
Repairs are performed on tear near the outer third of the Meniscus where a good blood supply exist, or on large tears that would require a near total resection. The torn portion of the Meniscus is repaired by using either plain suture or Suture along with bioinert devices which help to keep the torn edges together with very minimally invasive technique.
Meniscus tear are addressed according to the symptoms and the grade of the tear.
The repairability of any Meniscus tear will depend not only on the type of tear but also the zone in which they have occurred.
The tear in the red on red zone are repaired the most as this area has good blood supply on both sides of tear and have a good chance of healing as compared to Red on white or white on white where the blood supply is poor.
Similarly the type of tear also affects the repairability.
A longitudinal tear are best repaired as they show good healing potential while horizontal tears do well after good debridement alone. In some cases of horizontal tear repair is possible with mattress suture.
Radial tyres initially were thought to be non-repairable but with newer repairing technique they too have shown promising results.
The degenerative tears and flap tears which are generally a result of wear and tear over the period of time may not respond well to repair and often have to be trimmed. Here also where possible an attempt is made to repair in order to preserve the anatomy and function of the knee.
Three different kinds of surgical techniques are used to repair the meniscus
Post surgery patient is not allowed to put weight on the operated leg for 2 to 3 weeks. A long leg brace is given for immobilisation. Physio should begin immediately after surgery which includes
Gentle range of movement exercises are started around three weeks targeting 0 to 45° of flexion only. This is followed by partial weight-bearing walking and regaining full range of movement by end of six weeks. At this stage full weight-bearing walking and advance rehab is started in preparation for return to sports.
Meniscus repair should be considered in a young patient to improve the functional recovery of the knee joint if the Meniscus is repairable.